|
|
|
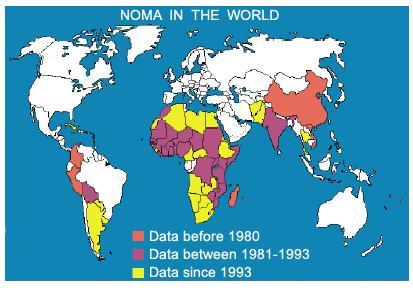
Map: WHO |
The following article is based on a report “The tragedy of Noma1”, prepared by Mr. Jean Ziegler, Vice-President of the UN Human Rights Council Advisory Committee. Unless otherwise noted, the quotes in this article are excerpted from this report by Mr. Ziegler.
Malnutrition and hunger are not only direct killers of children and adults all over the developing world. A lesser-known but horrible result of the negligence and callousness of the rich Western world is a cruelly disfiguring disease called noma (from Ancient Greek nomē "spreading of sores"), a scourge which is destroying lives in large parts of the developing nations.
Until very recently, little has been done in the world in order to deal with this awful disease, partly because it was mostly hidden away, due to the cruelly disfiguring facial sores that it causes.2 Impoverished parents, having children who were infected by noma, tended to hide their children away with their animals out of shame that they might bring dishonor on their families. It should be noted that noma is not even mentioned in a fact sheet on the top killer diseases in the developing world.
Nevertheless, for quite a few years now, private individuals as well as organizations have begun to deal with the victims of this horror. Treatment is possible at an early stage and surgery to restore destroyed faces is quite possible even at later stages. But the steps that have been taken so far are so few and far between that attention has to be drawn to the need for the World Health organization (WHO) to deal with it on a far larger scale.
The characteristics of noma
But let us first take a look at how and why this disease is spreading in poor parts of the world and then what can be done to make serious efforts to eradicate it, as has been done with other scourges such as leprosy, malaria, tuberculosis, measles and a multitude of other diseases that are now increasingly under control.
Noma (cancrum oris), which borrows its name from the Greek term “to devour”, is a devastating infectious disease that destroys the soft and hard tissue of the face. The lesion begins as a localized ulceration in the gingiva or the mucosa of the cheek or lip and spreads rapidly through the orofacial tissues. Untreated, the skin of the cheek or lip is typically perforated within a week of the start of the swelling. The gangrene of the facial tissue quickly spreads to other parts of the face such as the nose or an eye, leaving a terrible hole in the face. Noma leads to gangrene, sepsis and in 70-90% of cases, death. Most deaths are attributed to complications such as pneumonia, diarrhoea and septicaemia associated with severe malnutrition.
Survivors suffer threefold: disfigurement, functional impairment and social stigma.
This terrible, disfiguring and lethal disease mainly affects children aged 1 to 6, but late stages have also been observed in adolescents and adults. From studies in Nigeria it can clearly be seen that it affects children suffering from malnutrition and that affluent sectors of the population are spared. It is clear that it has to be seen as “a socioeconomic disease afflicting preferentially the deprived malnourished children in poor and mostly rural communities” (Reshma S Phillips et al. 2005)
Incidence of noma
The disease has virtually been eradicated from Europe and other countries with a high standard of living. It reappeared however in Nazi concentration camps (Bergen-Belsen and Auschwitz) during World War II, where food shortages were particularly prevalent. The disease has also been documented in HIV/AIDS infected patients from developed nations. A retired 68-year-old man from Great Britain was reported in a study from 2006 as suffering from noma.
However, the majority of people suffering from noma live in sub-Saharan countries. Cases are also reported from other countries in Africa, Asia and also in Latin America.
It is estimated (according to WHO in 1998) that 140,000 individuals yearly are infected by noma and that 100,000 of these are children between 1 and 7 living in sub-Saharan Africa.
Several factors make exact numbers difficult to obtain, one problem being that children with noma are often hidden by their parents, since noma is considered a social stigma, the same way that leprosy victims are generally seen as a shame to their families.
Because of a lack of appropriate information for the population in general and mothers in particular, noma tends to be perceived as a curse or as shame on the family whose child contracts it. It is certainly a powerful taboo that causes families to sometimes hide or isolate their children whose faces are disfigured by this disease with [their] animals. Furthermore, experts in the field have reported that noma is ignored and neglected by political authorities.
Causes and predisposing factors
Despite the lack of certainty in respect to the microbiology and pathophysiology, there is a wide consensus among experts that noma results from the interaction between three main elements: malnutrition, intraoral infections and compromised immunity.
Protein-energy malnutrition in combination with deficiencies in vitamins (A and B) and minerals are putting children at a high risk for attracting noma. A weakening of the immune system, often due to diseases (such as measles, malaria, tuberculosis, typhus, HIV) and poor oral hygiene also contribute to the development of the disease. Other risk factors are lack of safe drinking water and generally poor sanitation.
The treatment of noma
The WHO identifies four stages of the disease; noma can reach its terminal phase in the extremely short time span of three weeks. In the early stage, when the gingiva is bleeding and has lesions, impending noma can be treated in a manner which is “simple, effective, low-cost” with disinfecting mouth-rinses and daily food with vitamins. During the next phase, involving swelling of the face and fever, mouth-rinses, administration of antibiotics and nutrients supplementation is essential. These have been shown to prevent the progression from the initial ulceration to the acute phases of the disease, which presuppose emergency care and reconstructive surgery.
The death rate associated with noma is spectacularly high. However, with early treatment – oral hygiene, antibiotics and nutritious feeding, the rate can be lowered from 70 – 90% to approximately 20%. Thus, early recognition of the clinical signs of the disorder is vitally important, followed by proper treatment. Also, vaccination against infectious diseases such as measles would considerably cut the incidence of noma.
Improving the diet of malnourished children in risk areas could considerably lower the death rate and occurrence of this disorder. Bertrand Piccard3 , the founder of the organization Winds of Hope and president of the ‘No Noma - International Noma Federation’, considers that “the vaccine against noma, would be to feed all of Africa”. In more realistic terms, and in accordance with the Millennium Development Goals, ‘Médecins sans frontières’ (Doctors Without Borders) calculates that 2.76 billion Euro are needed to eliminate acute severe malnutrition of children. Put in perspective, 2.76 billion Euro represents a truly insignificant fraction of the economic recovery plans which have been approved in the last months by governments throughout the globe.
Quote from ‘NOMA: THE FACE OF POVERTY’
“Because Noma isn’t contagious, it’s nobody’s priority. Because it’s directly linked to malnutrition and poor hygiene, it’s seen as a problem without a solution. And yet it is a symbol. It is the symbol of the state of disparity in which our world is evolving, fractured into extravagant societies and starving populations, ultra sophisticated technologies and total destitution. It is also the symbol of our short-sightedness when we forget that humanity won’t be able to advance very far by leaving three-quarters of its population behind. Sounding the alarm is not a simple gesture of naïve solidarity, but truly of addressing the problem of safety for the future of our planet.” (Dr. Bertrand Piccard, President of the International NONoma Federation and President of the Winds of Hope Foundation)
The impact of the food and economic crisis
The effect of the aggravated food crisis due to the economic downturn must be addressed.
According to the Food and Agriculture Organization (FAO), as a result of the recent food crisis the number of chronically hungry people rose by 75 million in 2007, to reach a total of 923 million undernourished people. Today’s reality appears to be even bleaker than the one in 2007. A recent statement of the World Bank considers the number of undernourished to now exceed 1 billion. Looking at this data in a disaggregated manner shows that 89% of the 923 million chronically hungry people live in Asia and the Pacific and Sub-Saharan Africa.
The prevalence of malnutrition in both urban and rural households has dramatically risen due to the increased cost of staple foods, such as grains and vegetable oils. The situation in South Asia is particularly bleak.
Specifically in South Asia, the United Nations Children’s Fund (UNICEF) puts the number of hungry people in 2009 at 400 million, up by 100 million from the already unacceptable figure of pre-crises days. Moreover, of the 175 million children under 5 years of age living in the region, 45% are malnourished. By any measure this is the highest rate of malnutrition in the world, “eclipsing even Sub-Saharan Africa.” This picture is even more worrisome as it is generally acknowledged that the GDP growth rates of South Asia are twice as high as those in Africa, which means that surpluses during pre-crises years have not been used properly to tackle malnutrition of children.
Quoting UNICEF, the rate of malnutrition and hunger, intensified by the continued effect of the food, fuel and financial crises, “violate the rights of every child to food, education, good health and protection”. (UNICEF report, June 2009 – A Matter of Magnitude – The Impact of the Economic Crisis on Women and Children in South Asia)
In Jean Ziegler’s report, it is stated that medical studies have pointed to the link between the economic crisis, shortages in food and the incidence of noma.
Initiatives to Combat the Disease – WHO, national governments and non-governmental cooperation
In the African region, some progress has been achieved. It is essential to note the involvement of NGOs, charities and private individuals. These have been the driving force of the fight against noma, offering financial, logistical and medical support and assistance. To exemplify, the Noma Hospital in Sokoto, Nigeria (the only facility in Africa dedicated to the treatment of noma) has been established at the initiative and with the funding of ‘AWD-Stiftung Kinderhilfe’ from Germany, the ‘Dutch Noma Foundation’ and ‘Facing Africa’ from England with the cooperation of Nigerian authorities. To date, activities in the fight against noma have been implemented mainly in Africa, … It appears that the lack of funds made it impossible to expand the programs on noma to the Asian and Latin American continents, despite the fact that both regions have documented cases of noma.
Some steps forward have been made in terms of information and raising awareness on noma issues. With the help and financial support of a coalition of NGOs, the International Noma Day took place in Geneva on the 22 May 2008.
Raising awareness through any means available about this deadly disease is critical in this crisis period when malnutrition as the key risk factor has considerably increased.
While the goodwill and the competence of the WHO Africa Regional Office remains unquestionable, more must be done in the fight against this disease.…
Noma remains insufficiently prioritized at global and regional level. Despite having an associate mortality rate comparable with diseases such as acute upper respiratory infections, multiple sclerosis and appendicitis, noma does not appear in annual WHO reports. Moreover, noma is not listed among the major killers like malaria, diarrheal diseases, HIV/AIDS infection, measles, tuberculosis, and severe chronic malnutrition. However it is a complication of these diseases. As such and following plain logic, it should receive more attention.
It is simply logical that noma should receive more attention. It is not a contagious disease, but solely due to environmental causes and it would consequently be totally within our power to combat and cure. It is the clearest indicator of extreme poverty, but even though the mission of the World Bank is to reduce global poverty, this deadly disease does not sufficiently attract its attention. Noma was not even mentioned in the 1996 World Bank/WHO publication ‘The Global Burden of Disease’.
It is true that in 1998, the WHO Regional Committee declared the disease a priority on the African continent, but there is still not sufficient attention being paid to this cruel and stigmatizing disease. More real action is needed from international organizations.
The lack of public attention given to noma, the way this remains an anonymous disease can be seen as a result of the lack of data and WHO reports on the disease. The tragic effect is that fundraising and thus a capacity to combat the disease are being compromised by this lack of knowledge concerning this scourge that destroys human lives which could so easily be saved. Money and information are missing in a world where billions of dollars are given in the wink of an eye to huge banks where CEOs are drowning in money.
Let me remind you that over 100 000 people, the vast majority of which are children, die every year because of noma.4 And all it would take to combat this killer disease is eliminating hunger and malnutrition at a cost that would be a pittance compared to the trillions that are poured into the banks world-wide in the kind of welfare that is showered upon our financial institutions, instead of giving priority to the crying need for action to eliminate hunger, malnutrition and faulty sanitary conditions which are the causes of several perfectly avoidable diseases.
As a gripping demonstration of the priority given to banks before human beings, I repeat a passage from a recent interview with Jean Ziegler on the French information site BASTA!
“On October 12, 2008, the Heads of State of 15 countries that share the Euro, the 27 countries that make up the European Union, got together under the chairmanship of Ms Merkel and Mr Sarkozy at the Elysée Palace in Paris. In 3 hours and 30 minutes, they released 1.7 trillion dollars to improve the European banks’ lending capacity and to raise the level of auto-financing for those banks from 3 to 5%. The fact is that the UN has said that eradicating world hunger, eliminating the massacre of hunger, would cost 21 billion dollars over five years, less than one percent of the amount given to the banks.” (emphasis by SON)
Back to Mr. Ziegler’s report from the UN Human Rights Council Advisory Committee.
Noma is not addressed from a human rights perspective, despite being a human rights issue. This report insists on the links between noma and the right to food of the most vulnerable members of society, children living in poverty. Furthermore, the right to water, the right to adequate health care and not least the right to life are at stake. Addressing noma from a right to food perspective has implications for States and their obligations under international human rights law, as well as for international organizations in their response to noma and malnutrition.
Research into the causes and effective prevention and treatment of noma should be seen as a priority in solving the problems of injustice and inequality in today’s world. We already know that supplying nutritious food, vitamins plus minerals and vaccinations against the diseases that bring noma in their wake, measles, etc. can cure this disease at an early stage. Also, surgery can achieve miracles in cases where disfigurement has already gone too far to reverse the effects of the disease. It is of course essential to detect the disease at as early a stage as possible. This requires money and information among the populations at high risk.
RECOMMENDATIONS for what can be done to alleviate the curse of noma
Noma is killing, disfiguring, and destroying the lives of children. The persistence of noma in today’s world raises doubts not only about our morality, but it also comes to prove that the right to food of the children, the most vulnerable members of the international community is being severely violated. Malnutrition is the main predisposing factor of noma; malnutrition is easily treatable. To respect, protect and fulfill the right to food concerning the most vulnerable groups affected or at risk of being affected by the noma disease, the following steps should be taken:
- The fight against noma must be made a priority at international level. … In the view of the rise in malnutrition, all regions at risk must be included in the monitoring system.
- Inter-agency cooperation on the issue of noma must take place. … Noma should become integral part of the international response given by organizations such as FAO, WHO, UNICEF, the World Bank, etc. to the challenges posed by the food and economic crises.
- States must put in place national programs against noma or strengthen existing frameworks. States should allocate sufficient funds for prevention and information activities, as well as for nutritious food aid to individuals facing malnutrition. In case of lack of funds and faced with emergency situations, States have a legal obligation to appeal for international humanitarian aid. Not making such an appeal would be an encroachment on the right to food. Other States have a responsibility to cooperate as it is clear from Articles 2 and 11 of the International Covenant on Economic, Social and Cultural Rights and from customary international law.
Postword
The fact that this horrible disease is still continuing to wreak havoc in the developing world should be to the eternal shame of the wealthy countries – the other side of the coin where waste and luxury are the law of the land and overfeeding is the prevalent health problem. A few organizations such as the World Bank and the International Monetary Fund (IMF) are supposedly responsible for solving the ever-increasing and global problem of hunger. However, all they have done so far is to ever more enrich the rich countries and further strangle the poor countries that have been forced to humbly ask for loans to get out of their unacceptable living conditions. Instead of being enabled to give their people decent living conditions, these countries have been forced by the IMF to accept austerity measures, i.e. cutbacks in social spending and devaluation of their currencies, making the paying back of their loans even more hurtful and causing the living conditions of their citizens to deteriorate even further. So, as the poverty-stricken nations are gasping for breath, lacking food and clean drinking water and being robbed by the Big Transnational Corporations, while the rich 2% of the world population are gathering up further obscene wealth, the drive to the destruction of a decent and ethical cohabitation in this world is speeding up by the day.
-
HUMAN RIGHTS COUNCIL, Advisory Committee, Third session, 3-7 August 2009, Item 3 (b) of the provisional agenda.
-
For graphic illustration of disfigurement by noma go to ‘Facing Africa’ and ‘Project Harar Ethiopia’.
-
Bertrand Piccard and Brian Jones promised each other to dedicate their achievement (completing a non-stop balloon flight around the globe in 1999) to the children of the world and to use the media exposure and fund-raising potential of their fame to combat forgotten or disregarded suffering.
- The World Health Organisation (WHO) estimates that 140,000 new cases of Noma occur each year and of these, a mere 10% survive. That means that 126,000 die each year, mainly in sub-Saharan countries from Senegal to Ethiopia, a region known as "the Noma belt". (Facing Africa – NOMA)
Read her Biography and more of articles Siv O'Neall is an Axis of Logic columnist, based in France. Her insightful essays are republished and read worldwide. She can be reached at siv@axisoflogic.com.
by Siv O'Neall on Axis of Logic.