|
Axis of Logic
Finding Clarity in the 21st Century Mediaplex
Health/Medicine
An Extraordinary Success. Medical Internationalism in Cuba
By John M. Kirk. Counterpunch. Axis of Logic Commentary
Counterpunch
Sunday, Jul 28, 2013
Editor's Comment: In the article below, John M. Kirk provides a
comprehensive account of Cuba's breathtaking medical work around the
world based upon seven years of research
and some 70 interviews with Cuban medical personnel in Cuba and in other
countries. There is nothing we can add except perhaps to give a brief eye-witness account of the work of los médicos cubanos here in La
Victoria, a city of 200,000 people about 1 ½ hours west of
Caracas. The Cuban doctors provide free medical services in Venezuela's
Misión Barrio Adentro, a national health care program established by
President Chávez in 2005.
|
|
| Centro de Diagnóstico Integral (CDI) in La Victoria, Venezuela |
There are now 561 Medical Centers (Centro de Diagnóstico Integral or CDI),
583 rehabilitation facilities, 35 high-technology centers and six
thousand 712 modules (satellite clincis) of Barrio Adentro providing free health care
services across Venezuela. At the CDI here in La Victoria, where I myself have received treatment, the
Cubans provide diagnostic services with x-ray, ultrasound, ecosonogram,
voice diagnostics, endoscopy, electrocardiogam, ecocardiogram,
anatomical pathology and SUMA and Clinical Laboratories. The center is
equipped with an operating room, an infirmary, emergency room, a 24 hour
ambulance in service. Some of the services provided include emergency
services, outpatient treatment, sterilization, podiatry, opthamology
(laser surgery) optometry with free prescription glasses, chiropractic treatment, and
traditional medicine. In a separate building behind the one shown in the
photo Salas Rehabilitation Integral (SRI), qualified physical
therapists provide a full range of physical rehabilitation services
including PT in an adult and pediatric gym, hydrotherapy, thermo
therapy, cervical to lumbar traction and massage.
Cuban doctors
receive their training at Escuela Latinoamericana de Medicina (ELAM) in
Havana and graduate from a 6 year program, world renown for its
expertise in many different fields of medicine.
|
|
Escuela Latinoamericana de Medicina (ELAM), located on Avenue Che Guevarra in Havana
|
Medical students from
around the world receive their training at ELAM including those
receiving scholarships in the United States. On another personal note, my personal physician who provided me with excellent medical care for years, works at a large hospital of renown in Boston after attending medical school in Cuba.
|
|
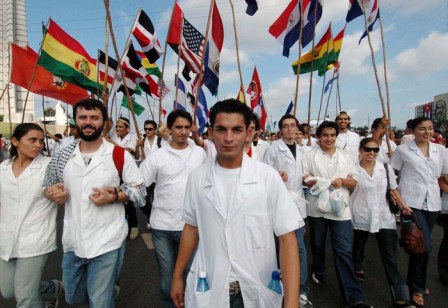
A group of US medical students who received their training at ELAM
|
The following report by John M. Kirk on Cuba's international medical system is the most comprehensive and accurate that either I or my co-editor (a Cuba specialist) have seen to date.
- Les Blough, Editor
Axis of Logic
| “What
is the secret of our approach? It lies in the fact that human capital
can achieve far more than financial capital. Human capital implies not
only knowledge but also-crucially important- political awarenes,.
ethics, a sense of solidarity, truly human feelings, a spirit of
sacrifice, heroism and the capacity to do a lot with very little”
- Fidel Castro Ruz, at the first graduation
of ELAM students, August 2005
|
The often-repeated quotation,
allegedly from Máximo Gómez that “los cubanos, o no llegan, o se pasan”
certainly applies to the programme of Cuban medical internationalism.1
Cuba certainly “se ha pasado” in terms of this policy: as of April 2012
there were 38,868 Cuban medical professionals working in 66
countries–of whom 15,407 were doctors (approximately 20% of Cuba’s
75,000 physicians).2In
Africa some 3,000 Cuban medical personnel are currently working in 35
of the continent’s 54 countries, while in Venezuela alone there are
approximately 30,000.3 But
that is only part of the story, since there are many other significant
facets to Cuban medical internationalism. In all cases it can be argued
that “human capital” is the most important common denominator.
This article, based upon seven years of research and some 70
interviews with Cuban medical personnel, both in Cuba and abroad, seeks
to provide a broad overview of the importance of Cuban medical
internationalism. There are several, very different, programmes of
medical cooperation that have been employed, and this article offers
basic data on their evolution and impact, as well as providing some
analysis of the rationale for their development.
Medical internationalism is not a recent phenomenon, and in fact can
be traced back to 1960–when Cuba’s first medical delegation flew to
Chile following a major earthquake there. The assistance was significant
because Cuba had strained diplomatic relations with the right-wing
Alessandri government at that time, emphasizing clearly the humanitarian
nature of the mission. A larger medical delegation was sent in 1963,
when Cuban medical personnel helped to establish the public health
system of Algeria, following its independence from France. Again, the
historical context is worth noting, since approximately one half of
Cuba’s 6,000 physicians had left the country, mainly heading for Miami.
In addition France, under President Charles de Gaulle, was one of Cuba’s
few remaining allies at that time—highlighting Cuba’s commitment to
humanitarianism rather than political gain. The significance of the
Cuban contribution at the time was well emphasized by the Cuban Minister
of Health, Dr. José Ramón Machado Ventura: “Era
como un mendigo ofreciendo ayuda, pero sabíamos que el pueblo argelino
la necesitaba incluso más que nosotros, y que la merecía”.4
(trans: "It was like a beggar offering help, but we knew that the
Algerian people needed even more than us, and they deserved it.") Human
capital, as defined by Fidel Castro, was even at this formative stage of
the revolutionary process once again the fundamental basis for the
decision to provide medical support.
The record of medical collaboration has continued, particularly in
developing and underdeveloped countries, and to date almost 135,000
health workers have participated in overseas missions. To put this in
context, Cuba currently has more medical personnel working abroad on
medical cooperation missions than all of the G-8 nations combined, an
astonishing record.
There are three basic stages in medical internationalism employed by
Cuba–the early years of the revolutionary process (best typified by the
sending of missions to Chile in 1960 and Algeria in 1963); the
mid-1970s (when Cuba, supported by the former Soviet Union and socialist
countries of Europe, developed a particularly strong programme of
collaboration in sub-Saharan Africa); and finally the period beginning
in 1990 after the nuclear meltdown in Chernobyl. This was followed by a
major increase in medical cooperation in the late 1990s, especially in
Latin America and the Caribbean, following the havoc caused by
Hurricanes George in Haiti and Mitch in Central America. This most
recent stage has resulted in numerous international health initiatives,
ranging from integrated health programmes (used in dozens of Third World
countries) and providing basic access to healthcare to millions of
people who often had never received any attention to the extremely
successful “Henry Reeve” Emergency Medicine Contingents which have been
employed in natural disasters.
While the record of medical internationalism is a long and
honourable one, the vast majority of Cuba’s contributions have been
since the late-1980s, the focus of this essay. One example is the
support given to victims of the Chernobyl nuclear reactor meltdown in
1986. In all some 26,000 victims (mainly children) have been treated at
the Tarará facilities since the first children arrived in March of 1990
(when they were received by President Fidel Castro, emphasizing the
importance given the initiative by the government). All medical
treatment for patients was provided at no cost to the patients, as was
their accommodation and food. This major humanitarian gesture is
particularly noteworthy since it was initiated just as the Soviet Union
was imploding, resulting in the loss of some 80% of Cuba’s trade, a
decline in GDP of some 30%–and the onset of the “Special Period” and its
many difficulties. From the Cuban perspective, the timing could not
have been worse. For many nations faced with such a profound crisis, it
would not have been surprising if the government had swiftly terminated
such a broad (and expensive) programme. Yet Cuba did not, again
displaying its human capital–and the commitment made to the children of
Chernobyl was respected.
|
|
| Dr. Julio Medina, Director and Dr. Xenia Laurenti Dilmes, Deputy Director for Medical Assistance |
After several visits to the facility and meetings with the patients
and Cuban medical staff it is clear that the attention given to the
children was excellent, and the facility–ably managed by Dr. Julio
Medina–has done an extraordinary job in difficult circumstances. At its
height some 350 people worked at the Tarará facility, which has a small
hospital, hundreds of buildings to house the patients, as well as
offering educational and recreational programmes for patients. The
children were first examined by Cuban medical personnel in their home
country, and usually stayed for 45-day periods, although children with
more serious ailments were treated by medical staff in various
specialized hospitals in Cuba. The objective was, quite simply, to offer
high quality medical and humanitarian support to children whose lives
had been badly affected by the impact of the nuclear meltdown. In all
21,874 children and 4,240 adults were treated in Cuba, of whom 19,497
were younger than 14, and the most common ailments were related to skin,
endocrinological and digestive problems.5(At
the time of writing Ukrainian President Victor Yankovich had agreed in
late 2011 to start paying for those costs, but to date has not initiated
payment, and sadly the programme has been placed on hold).
Also particularly noteworthy is Cuba’s role in training tens of
thousands of doctors from all corners of the developing and
underdeveloped world, both in Cuba and abroad. In the wake of the
horrendous damage caused in Central America by Hurricane Mitch in 1998,
the foundation of the Escuela Latinoamericana de Medicina (the largest
medical university in the world with an annual intake of over 1,500
students and with over 9,000 enrolled in the six-year programme) has
proved to be an extremely successful vehicle for providing medical care
for people who otherwise would have none.
|
|
ELAM Institute of Engineering and Biotechnology in Havana
|
To date approximately 10,000
physicians have graduated from ELAM. Over 20,000 foreign medical
students are also being trained through the Nuevo Programa de Formación
de Médicos Latinoamericanos–although this hands-on method is also being
used in a variety of countries, where training is adapted to local
conditions and specific needs. Cuban medical professors are teaching in
fifteen countries–and are especially numerous in Venezuela. In addition,
since the 1970s Cuba has assisted in the founding of medical schools in
several countries, including Yemen (1976), Guyana (1984), Ethiopia
(1984), Uganda (1986), Ghana (1991), Gambia (2000), Equatorial Guinea
(200), Haiti (2001), Guinea Bissau (2004), and East Timor (2005). The
role of Cuban medical professors is particularly important in Venezuela,
as noted later.
Hurricane Mitch (1998) in many ways was the catalyst for a
significant development in Cuba’s vastly increased approach to medical
internationalism. Some 30,000 people died in that natural disaster, and
the Central American leaders appealed to the international community for
assistance. Significantly, Cuba did not even have diplomatic relations
with the countries affected (several of which had traditionally
maintained a policy of hostility to the revolution), yet within days
sent 424 personnel to assist the affected areas. This would increase to a
maximum of 2,000, before settling at approximately 900 in the region.
What was particularly different about the mission in Central
America, however, was the decision to help the countries affected to
help themselves. Thus was born the central idea of ELAM, according to
which students from the region would be trained as doctors in Cuba so
that they could return and assist their own people. Cuban medical
personnel remained (and still remain), but have gradually seen their
numbers decrease as they are replaced by local medical graduates who
have been trained in Cuba. In November 1999 the Escuela Latinoamericana
de Ciencias Médicas (whose name was later changed to the Escuela
Latinoamericana de Medicina) opened its doors to the first students,
mainly from the affected region. Most of the students came from poor
backgrounds, and approximately one-half were women.
The Cuban approach to training foreign students at ELAM is based
essentially upon a commitment to train students who could not otherwise
attend medical school. The belief is that, since they are not from
privileged sectors, they are more likely to return to their communities
to work upon graduation, and help their people. In this way it is hoped
that the traditional “brain drain” (as graduates from Third World
medical schools head to First World countries where the salaries are
higher) would be reversed, and that a “brain gain” would result. It is
also noticeable how graduates from ELAM who, for a variety of reasons
cannot work in their own countries, have also volunteered to work in
other countries where there are underserved populations. The best
example is Haiti, where students from many Latin American countries are
currently working. The lessons of human capital in their six years of
training in Cuba have clearly been passed on to thousands of these
graduates.
In many ways representative of the Cuban level of collaboration
throughout the Third World is the broad outreach of Operation Miracle,
initiated in 2004. The origins of this wide-ranging ophthalmological
programme can be found in the challenges encountered in Cuba’s
outstanding literacy plan employed in several countries,6when
it was discovered that many people were unable to read mainly because
of existing medical conditions–mainly cataracts and glaucoma (both
easily treated with relatively minor surgery). They were unable to
participate in the literacy programme because of deficient eyesight. As a
result the revolutionary leadership decided to develop a programme that
would allow people to see again, and in particular this approach has
spread throughout Latin America. To take one example, in Bolivia alone
since 2006 more than 600,000 surgical operations have taken place,
mainly for Bolivians but also for citizens of other South American
nations bordering that country. Significantly, among the Bolivians
treated was Mario Terán, the soldier who executed Ernesto Che Guevara in
October 1967.
The success of this programme can be gauged by reading some of the
articles found in the “Oftalmología” part of the Infomed website.7In
the section “Más sobre Operación Milagro” there are dozens of articles
illustrating the enormity of this programme. To take just a few
examples: 15,000 Paraguayans have had their sight restored, 400,000
Haitians have benefited from the programme, 90,000 operations have been
carried out in Nicaragua, with almost 200,000 operations in Venezuela…
By October 2011 it was estimated by Dr. Reinaldo Ríos, medical director
of the Ramón Pando Ferrer ophthalmology hospital in Havana, that the
programme had treated over 2 million people in 34 countries of Latin
America, the Caribbean and Africa.8These
operations, carried out by Cuban physicians with Venezuelan support,
have been provided at no cost to the patient–the vast majority of whom
would otherwise have been unable to pay for these operations.
Another extremely important component of Cuban medical
internationalism in recent years is the role of the “Henry Reeve”
Emergency Contingent. The medical brigade (named after an American
participant in Cuba’s first war for independence) dealing with natural
disasters and serious epidemics was founded in September 2005 shortly
after massive flooding hit New Orleans as a result of Hurricane Katrina.
The Cuban government had offered to send 1,586 medical personnel and 36
tons of medical supplies to assist the people of the region, only to
have President George W. Bush reject the humanitarian gesture. Within
two weeks the “Henry Reeve” International Contingent had been formed,
with its goals outlined by Fidel Castro in his speech of September 19,
2005 at the graduation of medical students:
|
“This will take the place of
the Medical Force formed to help the people of the United States when
Katrina hit the south of the country with all its brutal force. Its aim
will not just be to help a certain nation, but to give immediate
assistance, with its specially trained staff, to any country that
suffers a catastrophe, particularly those that are hit by hurricanes,
floods or other natural phenomena of this severity”. |
The “Henry Reeve” contingent has been involved in 12 missions in
countries facing natural disasters, most recently in Chile following an
earthquake there. These have all taken place within the space of a few
years, a remarkable feat. The largest was to Pakistan (with some 2,250
members), although in many ways the most memorable has been that to
Haiti.
|
|
A team of Cuban doctors treating a patient in Haiti
|
Cuba has played (and continues to play) an enormously important role
in Haiti, both after the earthquake in January 2010 which killed
250,000 and in controlling the cholera epidemic which broke out nine
months later. Within two months of the onset of the epidemic almost
150,000 cases had been confirmed, with 3,333 deaths reported.9In
both cases Cuban personnel assumed the leading role in supporting the
Haitian people, and their efforts dwarfed those of the international
community. In fact Cuba had been providing a major medical presence
since 1998, when Hurricane George devastated the country. Some 500 Cuban
medical personnel had arrived at that time, and when the earthquake
struck twelve years later there were still 340 Cubans working in the
public health sector.
In terms of the cholera outbreak, the Cuban-led medical team was
bolstered by the arrival of ELAM graduates and upper level students. By
April 2011 there were 1,117 members of the Cuban medical brigade,
including 923 Cubans and 194 foreign graduates from Cuban programmes.
Together they had seen 2 million patients, operated on 36,000, and
delivered almost 35,000 babies. A further 465,000 Haitians had
benefitted from rehabilitation programmes.10
Again, their humanitarian efforts of the Cuban mission were (and are)
greater than those of all of the industrialized nations combined. To
date, however, these contributions remain largely ignored by the
international media.
Cuba’s role in Haiti has been exemplary. Not only did it provide by
far the largest medical contingent at the time of the earthquake, but it
also made the greatest contribution to stopping the cholera outbreak,
saving thousands of lives. Perhaps most important of all, Cuba is now
preparing Haiti for the future by establishing a public health system,
financially supported mainly by Venezuela and Brazil. Key to this will
be the role of Cuban-trained Haitian doctors, some 625 of whom had
graduated from ELAM by early 2011. Of these 430 were already working in
Haiti,11and later that year another 115 graduated from the Santiago de Cuba campus.
An equally important aspect (and in many ways a microcosm of Cuba’s
various medical internationalism programme) can be seen in its role in
Timor Leste. Cuban personnel arrived after an official request for
support in 2003, since as late as 2002 there were only 47 physicians in
the entire country. The initial role of Cuban personnel was to provide
badly-needed medical support in a country still recovering from its
independence struggle and invasion by Indonesian armed forces. Within
the first five years of the arrival of the Cuban brigade more than 2.7
million medical consultations had taken place, with an estimated 11,400
lives saved.
The next phase of Cuban cooperation in the country was to train
Timorese youth to become doctors, and take care of their own people. By
2008 “there were some 350 Cuban health workers in the region, with 870
East Timorese and more than 100 Melanesians and Micronesians engaged in
medical training”.12Most
received their basic training in Cuba, and then returned to Timor,
although increasingly the objective is to train them in their homeland,
where a Faculty of Medicine (staffed by Cuban professors of medicine)
was established in 2005. Once again the common theme of providing Cuban
medical support initially, and then developing local talent to replace
Cuban specialists and assume medical responsibilities, has been
successfully employed. Human capital has thus been transplanted to this
country, and is in turn being expanded to other small countries in the
South Pacific.
Comparable to the efforts in Timor Leste, although on a much larger
scale, has been Cuba’s medical cooperation in Venezuela, where at
present the largest contingent of Cuban medical personnel is found. The
contribution of almost 30,000 Cuban medical personnel in Venezuela
started in 1999 following massive flooding in the state of Vargas. Some
15,000 people died or disappeared, and within a week over 450 Cuban
medical personnel arrived to support the initiatives of newly elected
president Hugo Chávez. Four years later the municipality of Libertadores
in Caracas, noting the major public health deficiencies in the area,
appealed for medical support from Venezuelan doctors. Most refused,
citing concern over their personal security, leading President Chávez to
then approach Havana–and as a result in April 2003 Cuba sent 53 family
physicians.
It is important to recognize the determination of Chávez to use the
nation’s petroleum wealth for the benefit of the country as a whole, and
particularly marginalized sectors traditionally excluded from such
services. It is also worth emphasizing the level of bilateral
cooperation that resulted within just a few years. The original mission
to Libertadores was extremely successful, resulting in the decision to
expand the programme to the country, and ultimately the various stages
of Misión Barrio Adentro. The growth in the number of Cuban medical
personnel was extraordinary. According to Chávez, from just 53 doctors
in April 2003 this had increased by November 2010 to a situation in
which Cuban personnel were staffing 6,172 consultorios médicos
populares, as well as working in 3,019 dental positions, 459
ophthalomology posts, 514 Centros de Diagnóstico Integral clinics, 559
Salas de Rehabilitación and 28 Centros de Alta Tecnología.13
|
|
An ELAM Biotechnology Lab
|
In addition to Cubans treating Venezuelan patients in their own
country, over 51,000 Venezuelans have also received specialized medical
treatment in Cuba.14By
April of 2012 it is estimated that Cuban medical personnel had provided
over 745 million free medical consultations, with over 1.5 million
lives being saved.15(This
refers to people who, if adequate medical support had not been provided
and based upon traditional mortality patterns, would probably have
died). Preparing for the future, Venezuela is seeking to emulate Cuba’s
ELAM–and, with the support of Cuban medical professors, is training over
30,000 physicians. In February 2012 the first cohort graduated–8,150
specializing in Medicina Integral Comunitaria (MIC); a further 6,300 are
soon due to graduate, having completed the 6-year programme. At
present, according to Chávez, some 22,604 students are studying MIC in
Venezuela, and this will clearly make a significant contribution to the
public healthcare system.16It
is worth noting that none of this could have happened without strong
bilateral ties, and extraordinary Cuban cooperation in the national
medical system.
|
|
The first Venezuelan students to receive their masters degrees in Genetic Counseling
|
At times Cubans complain about their family doctor participating in
an internationalist mission, or having to walk further to the local
consultorio, because there are so many medical personnel are abroad. It
is worth noting, however that, while approximately 20% of Cuban
physicians are indeed working abroad, the ratio of doctor to patients in
Cuba is still probably the best in the world. A comparison with other
countries is pertinent in this analysis. In Canada there were 2.4
physicians per 1,000 population,17 and 2.4 in the United States in 2009, whereas in Cuba there were 6.7 in 2010, according to World Bank data.18
Moreover the distribution of medical attention to Cubans is far more
equitable than Canada (and indeed most industrialized countries,
including the United States), where a number of physicians work in the
private sector (making medical care inaccessible for many), and where
few physicians work in rural areas. While increased distances to visit a
médico de familia and longer waiting times might bother Cuban patients
(since so many physicians are in Venezuela), they are still in an
enviable situation–far better than any other country in the world in
terms of accessibility. As a result, the approximately 100,000 barrels
of oil received daily in Cuba (and with preferential prices) in exchange
for professional services, make this relationship mutually
beneficial–as anybody who remembers the dark days of the “Período
Especial” can attest.19
One of the most recent programmes undertaken by Cuban medical
internacionalistas has been the survey of the population of ALBA
countries to ascertain the level of physical and mental challenges of
their populations, carried out by hundreds of Cuban medical personnel in
member countries of ALBA. Cuba had already carried out a similar
medical survey within its own territory, arguing that this detailed
analysis was needed in order to both have a full understanding of
challenges facing individual members, and prioritize the medical needs
of these patients. In the case of Venezuela (where in 2008 Cuban medical
personnel–including a large pool of geneticists and social
psychologists– worked with local health brigadistas) in the Misión José
Gregorio Hernández, some 600,000 patients were identified as having
special needs–and the government moved to meet those specific concerns.
The purpose of these campaigns was thus not just to undertake a detailed
survey, but rather to undertake a scientific study to determine the
causes of the particular “discapacidad” and to provide the needed
assistance to the persons affected.
|
|
Cuban doctors returned eyesight to millions of Latin Americans, among them one individual who participated in the murder of Ernesto “Che” Guevara. Photo: Raquel Perez
|
Since 2009 other countries belonging to ALBA have also benefitted
from this detailed project. This was a massive undertaking, with over
71,000 specialists (Cubans together with specialists from each of the
countries involved) working on the project, going door-to door, and
visiting over 3,800,000 homes in Venezuela, Bolivia, Ecuador, Nicaragua
and Saint Vincent and the Grenadines.20
By July of 2011 a total of 1,017,464 people with special needs had been
identified in the ALBA countries where the research had been carried
out. In Bolivia this campaign was known as the Misión Moto Méndez (named
after a 19th century guerrilla), involving Cuban, Venezuelan and
Bolivian physicians, and as a result of the intensive campaign some
83,000 people with physical and mental challenges were discovered. The
Misión Solidaria Manuela Espejo had a similar goal–to undertake a
bio-psycho-social scientific study, in order to determine the causes of
the problems facing Ecuadorians, and the needs that they faced. In all
229 Cuban medical specialists and 129 Ecuadoreans visited 1,286,331
homes, and listed 294,611 persons with special physical or mental needs.
Significantly, by January 2012, a total of 265,515 technical supports
had been given to 135,254 of these people.21
Any one of these various programmes of medical cooperation would be
extraordinary for a country of the size and wealth of Cuba. Indeed no
industrialized country has ever attempted to undertake any one of such
ambitious healthcare initiatives. But to see the combination of so many
humanitarian initiatives being enacted is truly extraordinary. Just as
important is the recognition that these programmes have been ongoing for
five decades. In the case of Africa, to take just one example, while
there are currently some 5,500 Cuban professionals working there, almost
40,000 Africans have graduated from Cuban universities, and there are
currently 3,000 studying in Cuba.22
With justification Nelson Mandela summarized well the Cuban
contribution in his visit to Havana in 1991: “Venimos aquí con el
sentimiento de la gran deuda que hemos contraído con el pueblo de Cuba…
¿Qué otro país tiene una historia de mayor altruismo que la que Cuba
puso de manifiesto en sus relaciones con África?”.23
In the case of Latin America the data are even more surprising, since
particularly during the last twenty years Cuba has provided tremendous
levels of cooperation with countries of the region. Once again human
capital has been employed to the full–saving countless lives in the
process.
All of this poses the logical question: why does Cuba continue to
provide this far-reaching collaboration? One reason put forward is that
Cuba is seeking to exercise what is known in North American academic
circles as “soft power,” that is co-opting countries by showering them
with positive support and benefits in exchange for future considerations
from them. At first glance there would appear to be some validity in
this argument. Indeed it is obvious that Cuba’s programme of medical
internationalism–even in countries with which it had enjoyed difficult
diplomatic relations–has resulted in a clear softening of opposition by
those governments, and ultimately to a normalization of relations. After
all, how can you not have diplomatic relations with a country whose
doctors are saving thousands of your compatriots’ lives?
|
|
Cuban doctors providing treatment in Honduras where leftist President Manuel Zelaya was overthrown by the US-backed Honduran military in a coup d'état in 2009
|
It is particularly significant that Cuba has not provided medical
cooperation solely to countries with similar ideological convictions.
Mention was made earlier of the first mission to Alessandri’s Chile in
1961 and, also almost 40 years later, of the extensive Cuban
collaboration with Honduras and Guatemala (after Hurricane Mitch),
countries which had been strong US allies, and had traditionally
condemned Cuba. El Salvador, under a number of military governments, was
also a major ideological foe of the Cuban revolution, yet Havana did
not hesitate in sending 22 tons of emergency medical supplies following
an earthquake there in 1986. Likewise it sent a large medical delegation
in 2000 to assist when a major outbreak of dengue occurred. In addition
Cuba also provided medical support to Somoza’s Nicaragua after an
earthquake devastated the capital in 1972. No other Latin American
president had been as opposed to the Cuban revolution as Anastasio
Somoza, and indeed in 1961 he had allowed mercenaries to leave from
Nicaraguan ports in the abortive invasion of Playa Girón.
As an extension of this approach it is also argued that the Cuban
government pursues this policy to obtain votes of support at the United
Nations (which in 2011 saw 186 nations condemn the US economic embargo
of Cuba). In a May 2007 interview by the author and Michael Erisman with
Dr. Yiliam Jiménez, this argument was answered well: “Y si aun
aceptamos la perspectiva más cínica–o sea que Cuba manda médicos a
países pobres para ganar votos en la ONU, ¿por qué los países
industriales no hacen lo mismo? Lo más importante es salvar vidas–y eso
es precisamente lo que hace nuestra política”. Her argument is
completely correct. So far the lack of similar commitment to “salvar
vidas” on the part of the G8 nations is sadly absent, while consistently
Cuba has placed humanitarianism before ideology.
It is also abundantly clear that the major driving factor behind
these initiatives for decades has been the revolutionary leadership, and
in the particular the long-term vision of Fidel Castro, for whom access
to public healthcare has always been an extraordinarily important
issue–the most basic human right. From interviews with Cuban
policy-makers during the course of this research it is obvious that his
was the principal initiative in all of these programmes. The political
will to undertake these health campaigns, to mobilize human resources
and ensure adequate funding, thus came as a result of a political and
humanitarian decision taken by the presidency.
For a foreigner examining this complex, multifaceted phenomenon, it
is also clear that the development of a finely-tuned conciencia
socio-política on a national level is also an extremely important base,
allowing acceptance of these far-reaching policies. The successful
medical internationalism programme over the years has also supported the
sense of national identity, strengthening the profound sense of
nationalism and national pride that are extremely noticeable in Cuba.
This is supported by the Cuban Constitution itself which notes the
commitment to “el internacionalismo proletario, en la amistad fraternal,
la ayuda,a la cooperación y la solidaridad de los pueblos del mundo,
especialmente los de América Latina y el Caribe”. (trans: "The
proletarian internationalism, in the friendship, the aid, to the
cooperation and solidarity of the peoples of the world, particularly in
Latin America and the Caribbean."
The profoundly-rooted sense of international solidarity–which was
found as early as the struggle for independence in the late 19th
century–is also a key psychological factor. Cuba was assisted in the
second half of the 20th century by other acts of solidarity from
foreigners, from the key role of Ernesto Che Guevara to the economic
support of the countries of COMECON, and in more recent times from
Venezuela. The combination of decades of participating in
internationalist missions, or having friends and family members do so,
has resulted in a process of profound socialization in respecting such
humanitarian initiatives.
It is also true that the exportation of professional goods and
services is the largest single source of hard currency for the Cuban
economy, far outstripping tourism and nickel. Estimates for the amount
of income derived from medical services abroad range from $3 billion to
$8 billion annually. The most recent estimate is $5 billion, roughly
double the earnings from the successful tourist industry.24
Whatever the amount, it is still the largest generator of hard
currency for the government, and remains as a priority of the Cuban
government.
|
|
Foreign medical students in training at ELAM
|
With arguably a surplus of medical personnel (a position often
denied by members of the revolutionary leadership, who claim that there
is never have an excess of doctors), this use of trained medical cadres
is an enormously successful economic policy. The government of Raúl
Castro has moved to reduce some of the benefits earlier enjoyed by both
internacionalistas (lifelong financial supplements) and beneficiaries
(North American students at ELAM no longer study for free, the Ukrainian
government is expected to pay for treatment of children affected by the
Chernobyl implosion, and foreign students are now expected to pay for
further specialization). In addition the government has made it clear
that it is interested in expanding the medical tourism operations in
Cuba, and to send Cuban personnel to wealthy countries. This is
illustrated by the Cuban role in Qatar, where in early 2012 a 75-bed
hospital staffed by some 200 Cuban medical personnel was inaugurated in
Dukhan. In sum, while Cuba’s medical internationalism for poorer
countries remains intact, there is a growing determination to increase
profits from the exportation of medical goods (clearly seen in the
impressive growth of the biotechnology sector) and services.
On a personal level–that of the internacionalistas themselves–in the
course of interviews for my research it has been interesting to see the
explanations given by them for their involvement in missions abroad.
The majority explain that they participate in medical missions for
financial reasons since it allows them the opportunity to earn several
times their salary during their Internacionalista experience than they
would if they remained in Cuba. While it is extremely difficult to be
away from family for long periods of time, most welcome the chance to
earn a greater income, which allows them to purchase goods in Cuba that
otherwise they could not afford. (Most contracts are for 2-year periods,
although members of the mission generally return for a month midway
through their stay abroad). Since the start of the Special Period, there
is an inverted pyramid in terms of salaries, with those employed in the
tourist trade–even in positions where no further education is
required–earning far more than professionals with advanced degrees.
Internacionalista missions thus allow participants to redress in part at
least some of that imbalance.
Others have noted that the medical experience abroad in
underdeveloped countries represents an excellent opportunity for them to
develop their professional medical skills, since they deal with
situations that are often totally new to them. From malnutrition in
Gambia to gunshot wounds in Guatemala, the experience allows them to
expand their medical knowledge, to become better doctors and nurses.
Several others interviewed also refer to this experience as a kind of
rite of passage, something that almost all medical staff in Cuba do at
some point in their life. In sum, there are many different
reasons–ranging from genuine altruism to personal gain, from a
decades-long tradition of service to the possibility of
income-generation.
|
|
Public health has been one of the greatest accomplishments of the Cuban Revolution, which is not mere propaganda: Health indexes of Cubans are enviable when compared to the rest of the region. Photo: Raquel Perez
|
Whatever the motives of individuals or the revolutionary government,
there is no doubt that these five decades of medical cooperation have
made an enormous contribution to the wellbeing of the Third World. Any
one of these (many) significant medical contributions would be truly
noteworthy, particularly since Cuba is a small country, with severe
economic constraints. However, when seen in their entirety, they
represent a truly extraordinary contribution to the wellbeing of dozens
of countries around the globe. Writing in 2010, Julie Feinsilver offered
a succinct summary of the significance of this contribution. She noted
how Cuban internacionalistas have “saved more than 1.6 million lives,
treated over 85 million patients (of which over 19.5 million were seen
on house calls at patients’ homes, schools, jobs, etc.), performed over
2.2 million operations, assisted 768,858 births, and vaccinated with
complete dosages more than 9.2 million people”.25
Whether it be to Alessandri’s Chile in 1960, Somoza’s Nicaragua in
1972, or even George Bush’s United States in 1995 (when an offer of some
1,500 Cuban medical personnel in the wake of Hurricane Katrina was
rejected), the same commitment to assist humanity has been consistent.
Mention was made earlier of Fidel Castro’s speech at the founding of the
“Henry Reeve” Brigade. In it he also referred to the need to respond to
natural disasters, regardless of the ideology of the country: “Not
once, throughout the selfless history of the Revolution, have our people
failed to offer its supportive medical assistance to other nations in
need of this aid at times when catastrophes have hit them, regardless of
wide ideological and political differences, or the serious insults
received from the government of any of these countries”.
In essence Cuba has provided an example for the planet, showing how
its successful medical collaboration programmes have been far more
successful, and more far-reaching, than anything provided by all of the
G-8 countries’ efforts combined. For over fifty years Cuban medical
personnel have served the poorest and most neglected areas of the world,
going where other doctors refused to go. At present they are looking
after the wellbeing of some 70 million people. The root of this
contribution is the same “human capital” found in Chile in 1960 and in
each of the 66 countries where they are currently working. Indeed their
work–overlooked by the media in industrialized nations– puts the
“developed” countries of the world to shame…
John M. Kirk is a Professor in the Department of Spanish and Latin
American Studies at Dalhousie University, Halifax, Canada.
(all photos, related captions, in-text translatiosn and commentary by Axis of Logic)
Source: Counterpunch
NOTES
- This research project is
supported by funding from the Social Science and Research Council of
Canada. I would like to thank the Council for financial support. I would
also like to recognize the support of Dr. Víctor Manuel Rodríguez, of
the International Relations sector of MINSAP, and Dr. Arturo Menéndez
Cabezas, currently working in Barcelona, Venezuela. I would also like to
thank Emily Kirk, of the University of Nottingham, for her helpful
comments.
- Data provided by Dr.
Yiliam Jiménez, director of the Unidad Central de Cooperación Médica of
MINSAP, in a Prensa Latina report of April 3, 2012, “Colaboración médica
cubana, gratituidad y acceso universal”.
- “Alrededor de 5,500 profesionales cubanos prestan servicio en África,” Cubadebate, June 5, 2010.
- Cited in Piero Gleijeses,
Misiones en conflicto. La Habana, Washington y África, 1959-1976 (La
Habana: Editorial de Ciencias Sociales, 2002), p. 28.
- Data obtained from report
(“Pograma cubano de atención médica integral a niños relacionados con
el accidente de Chernobil”), received from Dr. Julio Medina, director of
the programme in Tarará, and from an interview with him in December
2011.
- The literacy programme
has been used in 29 countries, teaching basic literacy to 6.5 million
people, according to Pedro Rioseco, “Desarrollo exitoso del programa
alfabetizador ‘Yo sí puedo,’” Prensa Latina, May 24, 2012.
- See “Más sobre Operación Milagro”
- See “Misión Milagro ha beneficiado a dos millones de pacientes,” Radio Santa Cruz report, October 8, 2011.
- Conner Gorry, “Haiti One
Year Later: Cuban Medical Team Draws on Experience and Partnerships,”
MEDICC Review, vol. 13, no. 1 (Jan 2011), p. 52.
- See “Bruno Rodríguez en ONU: La reconstrucción de Haiti es tema pendiente,” Cubadebate, April 6, 2011.
- Gorry, p. 53.
- Tim Anderson, “Cuban
Health Cooperation in Timor Leste and the South West Pacific,” The
Reality of Aid: Special Report on South-South Cooperation 2010 (Quezon
City, Philippines: IBON, 2010), p.77.
- For further analysis, see
John M. Kirk, “Cuban Medical Cooperation within ALBA: The Case of
Venezuela,” International Journal of Cuban Studies, vol. 3, nos. 2/3
(Summer/Autumn 2011), p. 231.
- “Un paso gigante por la vida,” Juventud Rebelde, May 31, 2012.
- René Tamayo, “Una misión de vanguardia,” Juventud Rebelde, April 17, 2012.
- René Tamayo, “Primera graduación de médicos integrales comunitarios de Venezuela,” Juventud Rebelde, February 16, 2012.
- Patrick Sullivan, “Canada’s MD/Patient improves but low international ranking continues,” Canadian Medical Association, February 12, 2012 (See Accessed May 31, 2012).
- See “Physicians (per 1,000 people)” Accessed May 31, 2012). The website of the Oficina Nacional de Estadísticas in Cuba notes that in 2010 there were 76,506 physicians in the country, with an average of 1 physician for 147 patients.
- Dr. Jiménez has
summarized this relationship well: “We believe in fair trade. If that
means that we export a product that we have surplus of–in this case
educational goods and services–to a friend at a reduced price, and they
export to us at favorable conditions something that they have in
abundance–petroleum–what is wrong with that?”. See John M. Kirk and H.
Michael Erisman, Cuban Medical Internationalism: Origins, Evolution and
Goals (New York: Palgrave Macmillan, 2009), p. 186.
- Data taken from two
reports, “Destacan resultados de estudio sobre discapacidad en países
del ALBA,” Cubadebate, July 7, 2010 and “Exitoso estudio cubano de discapacidad en países del ALBA,” November 27, 2010.
- Data taken from “Misión solidaria Manuela Espejo,” n.d., issued by the Office of the Vice-President of Ecuador.
- Data taken from comments by Deputy Minister of Foreign Affairs, Marcos Rodríguez in “Alrededor de…,” Cubadebate, June 5, 2012.
- Gleijeses, p. 458.
- Fernando Ravsberg, “May Day in Cuba: The Doctors Out in Front,” Havana Times, May 2, 2012.
- Julie Feinsilver, “Cuba’s Health Politics: At Home and Abroad,” Report prepared for the Council on Hemispheric Studies, March 2010.
|
|
|